
Follistatin 344 is an investigational compound. No injectable follistatin product carries FDA approval, and what human data exists comes from a handful of gene therapy patients rather than from the peptide vials sold online. Every figure cited below traces to a primary source. Last reviewed: June 2026.
There is a useful way to sort the claims made about Follistatin 344, and it has nothing to do with how exciting each one sounds. The molecule shows up in three very different settings in the scientific literature: engineered mice, gene-therapy trials in monkeys and in sick patients, and the peptide vials marketed for self-injection. Those three settings do not share a dose, a delivery method, or, in most cases, a species. Reading the material tier by tier, rather than letting the most dramatic number bleed across all three, is the organizing idea behind this piece.
Orientation: what the compound is and isn’t
Follistatin is a protein the body makes on its own. “Follistatin 344,” or FS344, is a specific 344-amino-acid version of it. Its relevant job, for this discussion, is straightforward: it binds myostatin, the protein product of the GDF-8 gene that acts as a brake on muscle growth, and holds it inactive. A 2004 paper in Developmental Biology documented this binding directly, showing follistatin complexing with myostatin and blocking its inhibition of myogenesis, the process by which new muscle forms [3]. Take the brake off, and the conditions for growth improve. That mechanism is well established and not in dispute.
The “344” label became attached to commercial products almost by accident. FS344 is the exact isoform researchers packaged into a viral vector for gene therapy trials in muscle-wasting disease. The name migrated from the lab notebook to the product label. What did not migrate, notably, is the delivery method, and the delivery method turns out to be the whole story.
The evidence, arranged by what it can actually support
Grading each layer of the literature by what it demonstrates, rather than by how often it gets quoted, produces a fairly stark picture.
| Evidence tier | What it shows | What it does not show |
|---|---|---|
| Myostatin knockout mice [1] | Removing myostatin produced individual muscles roughly 2 to 3 times larger than normal | That an injected peptide reproduces this in adult humans |
| Follistatin knockout mice [2] | Follistatin is essential across many tissues; deficient pups died within hours of birth | Anything reassuring about adding extra follistatin to a healthy adult system |
| Binding mechanism [3] | Follistatin sequesters and antagonizes myostatin | A dose, schedule, or human outcome |
| Macaque gene therapy [4] | AAV1-FS344 delivery raised muscle size and strength durably, with no abnormal changes to major organs | That injecting the protein or peptide directly does the same |
| Becker muscular dystrophy trial [5] | Six patients, gene therapy; some six-minute-walk gains up to roughly 108 meters at 6 months; reduced fibrosis; no serious adverse effects | Efficacy or safety for healthy adults building muscle |
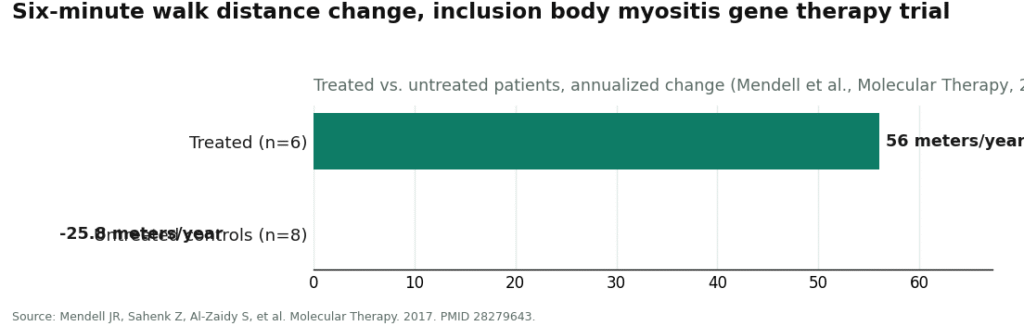
| Inclusion body myositis trial [6] | Six treated versus eight untreated; walk distance changed +56.0 m/yr in the treated group versus -25.8 m/yr in untreated controls, p = 0.01 | Benefit outside that disease, or from an injected peptide rather than gene therapy |
| Injected FS344 peptide in healthy adults | No published controlled trials exist | Everything a buyer might assume about it |
Look at the right-hand column. Every entry graded “strong” belongs to pure genetics or to gene therapy delivered under clinical supervision. The row that describes what people actually purchase online is empty. That is simply where the published record stands, not an editorial verdict layered on top of it.
See also: 9 Places I Actually Looked at for GLP-1 and Peptides Together (And What I Found)
The macaque study, and what it does not license
The most frequently cited figure in this space comes from Kota and colleagues, published in Science Translational Medicine in 2009 [4]. It is a real and genuinely encouraging result: researchers injected an adeno-associated virus carrying the follistatin gene, AAV1-FS344, into monkey quadriceps and observed durable increases in muscle size and strength, with no abnormal changes to the morphology or function of major organs over long-term expression [4].
What tends to go unmentioned is that the monkeys were not injected with follistatin protein. They were injected with a virus that reprogrammed their own muscle cells to manufacture follistatin continuously, from within. The dose, the duration of expression, the pharmacokinetics, and the safety profile of a one-time viral gene delivery do not transfer cleanly to a person drawing reconstituted powder into a syringe on a recurring schedule. The molecule named on the label is the same. The intervention is not.
The human data, at its actual size
Two published trials, from the same research group, make up essentially the entire human record for FS344. The first, in Molecular Therapy in 2015, treated six patients with Becker muscular dystrophy using bilateral quadriceps injections of AAV1.CMV.FS344. Results were mixed: some patients in the higher-dose cohort gained up to roughly 108 meters on the six-minute walk test at six months, others did not improve, and biopsies showed reduced fibrosis and signs of regeneration, with no serious adverse effects reported [5]. The second, in Molecular Therapy in 2017, applied the same gene therapy to sporadic inclusion body myositis: six treated patients against eight matched untreated controls, with the treated group gaining an annualized 56.0 meters of walk distance while controls declined by 25.8 meters, a difference reaching statistical significance at p = 0.01 [6]. Both trials trace back to a single registered Phase 1 safety-and-feasibility study run at Nationwide Children’s Hospital [7].
Put together: roughly a dozen patients, total, all with degenerative muscle disease rather than ordinary physiology, all receiving a one-time viral gene delivery rather than a repeated peptide injection, with individually mixed responses. That is a legitimate, promising early signal in a specific patient population. It is not evidence that a healthy adult injecting reconstituted FS344 will gain muscle, and the existing studies do not address whether repeated peptide use over months would be safe.
On dosing, honestly
Anyone arriving at this topic usually wants a number: so many micrograms, this many times a week. None exists in the published research, and inventing one would misrepresent the science. The trials that produced results used a fixed quantity of viral vector delivered once, not a recurring peptide dose. There is no published pharmacokinetic profile for injected FS344 peptide, no established cycle length, and no dose-finding study in healthy people. Part of the reason researchers turned to gene therapy in the first place is that follistatin is a large protein with a short half-life and effects across many tissues, which makes repeat injection a poor delivery strategy on its own terms [2][4]. Any specific microgram protocol attached to a vial online reflects community convention, not a research finding, and that distinction matters more than it sounds.
What the knockout mice quietly caution against
One further data point deserves weight precisely because it cuts against the enthusiasm. When researchers produced follistatin-deficient mice in 1995, the animals did not simply end up with less muscle. They showed skeletal defects, abnormal whiskers and teeth, reduced diaphragm and intercostal muscle, taut shiny skin, and died within hours of birth, unable to breathe [2]. That result describes a protein woven into development across multiple organ systems. It does not prove that supplementing follistatin in an adult causes harm, but it is a solid reason to treat “more follistatin, broadly” as a systemic intervention with genuine unknowns rather than a single clean lever on muscle alone.
The providers, if someone is going to pursue this anyway
Given how thin the human evidence is, the more consequential decision for anyone still considering Follistatin 344 is not which vial to buy but which route to buy it through. Obtaining an investigational compound through a licensed clinician who reviews medical history, decides whether a prescription is appropriate, uses a licensed compounding pharmacy, and follows up over time is a materially different proposition from wiring money to a vendor selling a “research use only” vial with no medical oversight attached. FormBlends operates on that supervised, prescription-based, pharmacy-dispensed model. It lists Follistatin 344 as a compounded option, states plainly that the compound is not FDA-approved, and leaves prescribing decisions to independent licensed providers rather than to the platform itself. Naming it here is not an endorsement of using the compound. It is pointing at the one structural difference that adds real accountability to a decision the underlying data cannot make safe on its own.
The bottom line
The mechanism is solid. The mouse genetics are solid. The gene therapy data, in both monkeys and in a small group of patients with muscle-wasting disease, is real. Roughly a dozen human beings have received the compound in any published, controlled setting, all through gene therapy, all in disease, with mixed individual results. Controlled trials of the injected peptide in healthy adults number zero. An established dose for that peptide does not exist. FDA approval does not exist. Holding all of those facts at once gives a more accurate picture of Follistatin 344 than the marketing pages that lead with the two-to-three-times figure from mice and stop there.
The compound may eventually earn a defined medical role. As of today, the exciting evidence and the evidence for the product actually being sold are not the same thing.
What people tend to ask
What does Follistatin 344 actually do in the body?
It binds and neutralizes myostatin, a protein that limits muscle growth, along with several other TGF-beta family signaling molecules including activin. In animal studies, reducing myostatin signaling this way produces substantial muscle hypertrophy. The pathway is thought to work similarly in humans, but injecting the protein directly has not been shown to reproduce those animal results, partly because the protein degrades quickly and does not appear to reach muscle tissue in useful concentrations without a delivery system like gene therapy.
What are the realistic side effect risks of Follistatin 344 sold online?
The honest answer is that the side effect profile in humans is largely unknown, because controlled human data on injected Follistatin 344 is close to nonexistent. Theoretical concerns include disrupted reproductive hormone signaling, since follistatin also suppresses FSH, and effects on cancer cell proliferation, since some tumor types upregulate follistatin naturally. Separate from the biology, peptides sold through research-chemical channels also carry contamination and misdosing risks that have nothing to do with the compound itself.
Is Follistatin 344 legal to buy and use?
In the United States, Follistatin 344 is not approved as a drug, so it cannot legally be sold for human use. Many vendors label it “for research use only” to sit outside FDA oversight, but buying it with the intent to inject it is a genuinely gray-to-red legal area. WADA has banned it in sport. A physician-supervised compounding route, such as through a licensed pharmacy like FormBlends, sits under a different regulatory accountability structure than the research-chemical market does.
Does the evidence actually support Follistatin 344 working for muscle gain in healthy adults?
Not currently. The human evidence for injected Follistatin 344 in healthy people is close to nonexistent. Gene therapy trials in patients with muscular dystrophy and inclusion body myositis have shown a real signal, but those relied on intramuscular viral delivery, not a subcutaneous peptide injection. Extending those disease-specific gene-therapy results to a healthy person injecting reconstituted powder at home is a leap the current data does not support.
References
- McPherron AC, Lawler AM, Lee SJ. Regulation of skeletal muscle mass in mice by a new TGF-beta superfamily member. Nature. 1997. PMID 9139826. https://pubmed.ncbi.nlm.nih.gov/9139826/ . Myostatin knockout mice show muscles 2 to 3 times larger; myostatin is the negative regulator of muscle growth.
- Matzuk MM, Lu N, Vogel H, et al. Multiple defects and perinatal death in mice deficient in follistatin. Nature. 1995. PMID 7885475. https://pubmed.ncbi.nlm.nih.gov/7885475/ . Follistatin-deficient mice show reduced diaphragm and intercostal muscle, skin and skeletal defects, death within hours of birth.
- Amthor H, Nicholas G, McKinnell I, et al. Follistatin complexes Myostatin and antagonises Myostatin-mediated inhibition of myogenesis. Developmental Biology. 2004. PMID 15136138. . Characterizes the follistatin-myostatin binding mechanism.
- Kota J, Handy CR, Haidet AM, et al. Follistatin gene delivery enhances muscle growth and strength in nonhuman primates. Science Translational Medicine. 2009. PMID 20368179. . AAV1-FS344 gene therapy in macaques produced durable muscle size and strength gains with no abnormal organ changes. Gene therapy, not protein injection.
- Mendell JR, Sahenk Z, Malik V, et al. A phase 1/2a follistatin gene therapy trial for Becker muscular dystrophy. Molecular Therapy. 2015. PMID 25322757. . Six patients, AAV1.CMV.FS344; some six-minute-walk gains up to about 108 m at 6 months in the higher dose; reduced fibrosis; no serious adverse effects; mixed response.
- Mendell JR, Sahenk Z, Al-Zaidy S, et al. Follistatin Gene Therapy for Sporadic Inclusion Body Myositis Improves Functional Outcomes. Molecular Therapy. 2017. PMID 28279643. . 6 treated vs 8 untreated; walk distance +56.0 m/yr treated vs -25.8 m/yr untreated, p = 0.01.
- ClinicalTrials.gov. Follistatin Gene Transfer to Patients With Becker Muscular Dystrophy and Sporadic Inclusion Body Myositis (rAAV1.CMV.huFollistatin344), Phase 1, Nationwide Children’s Hospital. NCT01519349. . Registered trial record for the human FS344 gene therapy work.
- U.S. Food and Drug Administration. Cellular & Gene Therapy Products. . Regulatory framework establishing that gene therapy and biological products require approval; no approved follistatin product exists.
Written by Bruno Moreno, features writer. Cross-checking the claims against the primary sources. Last reviewed June 2026.
Not a substitute for medical care. Bring any new treatment idea to your healthcare provider first.
